
Make sure everyone knows the aim of your engagement
When working with consumers, make it clear:
- What can change and what cannot
- What the aim of the engagement is (why are you engaging people and how will this help your project?)
- What the role of consumers is
- How the engagement activity or committee works
How to identify consumers and their engagement needs
You can identify consumer stakeholders by looking at:
- National and state data collections (e.g. Australian Bureau of Statistics, Australian Institute of Health and Welfare)
- Local data, to get an idea of the population demographics in your area – like your local Primary Health Network Needs Assessment, or local health service strategic planning documents
- Your own service data
- Research on groups underutilising services
- People who have recently used or currently using your service
- People already involved in your project during the planning stage
Actively seek involvement from those not using your service. Think about whether you can engage people through other health and social organisations or community groups (e.g. RSLs, Men’s Shed, parenting groups, support groups, sporting organisations).
Give yourself enough time to build relationships and engage properly, especially if working with groups who do not engage often with health services.
Cater to consumer engagement needs
Consider reasons why people may not be able to engage in particular activities – like the timing of engagement activities, not feeling culturally safe, lack of trust in health service, discomfort of being in health facilities, distance to health facilities, work/childcare commitments, etc. Adapt your engagement methods to be more inclusive. You may need to consider:
- Timing (e.g. not around holidays, multiple sessions at different times of the day, providing enough time for people to do activities around their busy schedules, after hours engagement)
- Location (some locations may not be appropriate or be too far to travel). You may need to engage with people in their own space or community
- Multiple methods of engagement to suit different groups: online, face to face, email, phone call
- Will you need multiple engagement sessions with different groups or a mix of different stakeholder groups? Will a mix of groups e.g. patients and nurses, work in the same session or will you need multiple sessions?
- Providing incentives
- Working with activities already happening – does the group you want to engage already meet for other reasons?
- How we engage – you might be used to formal agendas and presentations, but community members may not be used to working this way. Informal, flexible agendas and interactive activities may be more appropriate.
Download this PDF about Practical implementation of flexible engagement to suit the needs of the community.
Make your engagement culturally safe for Aboriginal and Torres Strait Islander people
- Work with your service/organisation’s Aboriginal and Torres Strait Islander Unit to plan engagement that meets the needs of local communities
- Do cultural safety training
These guidelines and principles refer to research but can also be applied to broader engagement:
Use the right methods for engaging people
The level of engagement you use will dictate the tools and methods of engagement.
Here are some examples for each level of engagement from A Guide for Health Staff – Partnering with Consumers, Health Consumers Queensland, and the Western NSW PHN Community Engagement Framework
Share (inform)
- Patient/carer information
- Community engagement conference
- Fact sheets
- Website
- Social media
- Newsletters
- Public displays
- Event
Acknowledge (consult)
- Feedback on publications
- Focus groups
- Reference groups
- Surveys
- Pubic forums
- Interviews
- Community representatives on committees
- Evaluation surveys
Explore together (involve)
- Reference groups
- Patient/carer forums
- Safety and quality meetings
- Improvement working groups
Build(collaborate)
- Co-design
- Advisory groups
- Planning workshops
- Participatory decision making
Enable (empower)
- Citizen juries
- Delegated decisions
- Community appointed management committee
Here’s an example
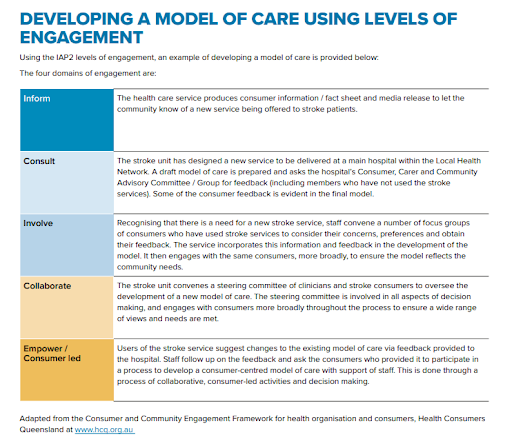
Source: Engaging with Consumers, Carers and the Community – Guide and Resources, SA Health
How many consumers should I engage with?
- Depends on the type of activity you are doing and the diversity of consumers that use your service
- For feedback on basic written health information, aim to get feedback from at least 5 consumers. You can use the tools on this page to help you.
- For activities involving the review or redesign of how services work you will need more people
- For larger activities requiring ongoing involvement from consumers, aim to recruit at least 2 people, preferably more if you are working at higher levels of engagement.
- Health Consumers Queensland recommends that at least 2 consumer representatives are recruited for each activity in order to provide support to each other, provide skills development and mentor more people to take on these roles.
Engagement can take weeks after you consider organization approvals, recruitment, planning, etc. Allow at least 6 weeks, depending on the level of engagement you are seeking. Higher levels of engagement, which may require multiple activities, will take longer.
Should I pay consumers for their time?
Besides the other costs that come with engagement activities (venue hire, catering, facilitator fees, etc.), you need to plan for remuneration of consumers involved with your project.
Consumers provide their valuable time to help with your project, and this input should be recognised.
Your organisation or service may have a policy about consumer remuneration.
There is no national agreement on how much to pay people for their time. When deciding on the amount, consider:
- Transport costs
- Time away from work
- Costs of other arrangements (e.g. babysitters)
- People’s expertise
How do I recruit consumers?
Different methods of recruitment have pros and cons. These include:
Expression of Interest (EOI)
- Open to a broad range of people
- Allows you to gather demographic details
- Potentially brings in people who have not partnered with your health organisation before
Direct recruitment (asking someone in particular)
- Quick
- Very specific circumstances match perfectly with an opportunity
- Decreases the diversity if using a “professional” consumer rep
- Gives the impression that we only want to work with certain people
Asking people who have recently used your service
- People have experience of your service (could also limit to people that have had multiple experiences with the service – e.g. second baby, multiple admissions)
- Easy to access
- May need to get consent from people to contact them after discharge
Through other organisations or services
- Levers existing relationships people may have with health professionals
- Need to get buy in from other services/organisations
- Consumers may not feel comfortable engaging without the person from the other service/organisation present
Whatever you choose, follow up with everyone that engages with you or the project in some way, even if they don’t end up being involved, and let them know what you are doing and the outcomes of the project.
Where to advertise
Advertise for specific projects or roles via:
- your website
- websites of other organisations
- e-newsletters of community health organisations
- community newspapers
- notice boards of health and medical centres (clinics, hospitals)
- social media
- consider approaching disease-specific organisations or general consumer health groups.
- consider engaging already registered consumers to recruit peers.
Source: WAHTN Involving Consumers in Health Medical Research Handbook
What information should I include in an Expression of Interest?
- Address why consumers would want to be involved
- Aims of the project
- Information about the service this project is based in
- Who else is involved in the project (other stakeholders)
- Which group of people you want to involve in the project (target group)
- If any skills or experience is required
- The scope of the consumer’s role
- Commitment required from consumer (time, travel, preparation)
- Timeline of the project
- Reimbursement
- Contact details
Considerations for application form:
- Limit questions in EOI application – aim for no more than 6 questions
- Use plain English to write questions
- Provide multiple methods for completing the EOI (online, phone, paper)
- Keep it open for long enough, but not too long (aim for 2 weeks)
- Communicate with unsuccessful applicants
- May not adequately capture any conflicts of interest or personal agendas
Source: A Guide for Health Staff – Partnering with Consumers, Health Consumers Queensland
Do I have to get people to fill out any forms?
Check with your organisation or service. Some examples of forms you may need people to complete before participating in an engagement activity include:
- Privacy agreements
- Code of conduct
- Consent forms
- Media consent forms
Practical tips for effective engagement
- Spend time making sure everyone involved has a clear understanding of the scope and aims of the process and what they are being asked to do. Consumers may not understand how an activity or group works and how much engagement or input you want.
 Provide support for people participating in activities, e.g. give people a chance to join a practice online meeting if they are new to this, meet people or phone people early to explain the process in more detail, offer to go over project documentation with people.
Provide support for people participating in activities, e.g. give people a chance to join a practice online meeting if they are new to this, meet people or phone people early to explain the process in more detail, offer to go over project documentation with people.
Source: WAHTN Involving Consumers in Health Medical Research Handbook- Do not use jargon in your engagement activities or any documents you send out
- Make it comfortable
- Don’t be too formal – even group work should have an informal feel to it
- Be honest if you don’t know something or are worried about something
- Do short sessions (maximum of 2 hours) if possible
- Break up activities with food and energiser games
- Each method of engagement must have a way for capturing ideas and outcomes (e.g. dedicated note takers, writing ideas down and collecting these notes, recording, photographs).
- Participants should be given the record of outcomes to review so they know their input has been captured correctly
- Keep people in the loop about the outcomes of the engagement and the process
- Evaluate the process as well as the outcomes (e.g. changes resulting from engagement, building capacity, barriers encountered and solutions, learnings about the system, which methods of engagement work best, what risks needed to be managed)
- Celebrate the value of everyone’s contributions
- Be creative – you aren’t limited to workshops and surveys
- Group engagement is usually preferred, as long as people feel welcomed. Make sure people are not put on the spot in a group setting and give people other options for engaging if they do not feel comfortable in groups
- If you want feedback on something quite complex you need to give people time to think about it (e.g. you might have a workshop and then send a follow up email asking for feedback, or hold another session)
- If calling on the phone – don’t use a private number, or tell people when you will call
- Limit the amount of information you send out digitally – people may not have large devices to read long documents on
- Don’t ask people to print anything – if someone needs something in hard copy, mail it to them.
- Balance the demand you place on participants with enough information for them to give meaningful feedback
Facilitation
A facilitator:
- is neutral
- encourages participation
- builds an understanding of the problem
- encourages and guide the process, does not engage in it
- explains the process of engagement/instructs people through certain activities
- keeps discussion on track and within scope
- summarises main points and converges different ideas
- summarises progress during the meeting visually
- keeps the meeting on time.
Tips for facilitators:
- use evidence as a conversation starter
- make it fun and engaging – games, role plays, mapping exercises, pictures – get people up and doing something other than listening and discussing
- keep meetings short or break them up with energiser activities or food breaks
- practice your facilitation skills with colleagues
- get someone else to facilitate if this is not your strength.
 Example – Kidney Health Plan design focus group (submitted by Graeme Turner, Nurse Practitioner, Northern NSW Local Health District)
Example – Kidney Health Plan design focus group (submitted by Graeme Turner, Nurse Practitioner, Northern NSW Local Health District)
Recording outcomes and actions during the engagement
Depending on the type of engagement you use, you should record the methods you used and the outcomes.
Some ways to do this:
- Minutes of meetings
- Table of feedback and actions against suggestions
- Survey responses/report
- Workshop summaries
- Photos of engagement activities
- Written summaries of activities
Action plans
- Include any suggestions/feedback/requirements recorded from your engagement and whether these were acted on and how.
- If they were not, include a reason why.
- Share this with the people involved in your engagement activity.
Surveys
- Cheap
- Good for quantitative data
- Generally get low response rates
- No opportunity to ask for clarification on any issues that comes up
- Low level of influence from consumers on outcomes from survey
- Are surveys the best way to engage people about your project?
- Will your survey delivery method exclude certain population groups?
- How will you distribute the survey?
- How will this distribution method impact completion rate; bias; staff time?
- How will you ensure that a diverse sample completes the survey?
- What response rate do you need for reliable information?
- Do not selectively survey your population. Either randomly choose people to send a survey, or send to all consumers accessing your service
- You will likely get a higher completion rate if people are filling in the survey at the health service, but this will introduce some bias
- Provide a quiet, private place for people to complete surveys
- Arrange for support staff to offer help to complete the survey
- If you have a captive audience, investigate ways to use technology to improve engagement
- Let people know that you will ask them to complete a survey. If people can put a face with the reason for doing the survey they are more likely to complete it.
- Check for existing surveys (e.g. Patient Reported Measures, Bureau of Health Information)
- Really think about what information you want to get out of the survey, and what you are going to do with that information. Is a particular question going to give you useful information, or just “nice to know” information?
- Keep it as short as you can
- Use plain language in all questions
- Make sure you are only asking one question in each question
- Check for bias – make sure you’re not asking leading questions
- Limit the number of open ended questions you have on a written survey
- If using questions that have a scale for the answer (e.g. strongly disagree to strongly agree, or poor to excellent, etc.), include an “I’m not sure”, or “this does not apply to me” option where needed
- How are you administering the survey – online? On paper? On a tablet? In the clinic or at home? This will affect the format and the questions.
- How will you enter and analyse the data so it is as neat and easy as possible?
- Unless looking at individual health outcomes, make surveys anonymous or de-identified
| Do not | Do |
|---|---|
| Write questions with ambiguous meaning | Be specific |
| Please tick the following community safety activities you know about. | Please tick which of the following community safety activities you have participated in this year |
| In the past month, how many times have you visited a doctor? | We would like to understand how often you have visited a licensed medical professional, including dentists, psychologists, chiropractors, and nutritionists. In the past 30 days, how many times have you visited a medical professional? |
| How would you rate your health? | Do you think you eat enough vegetables? (I eat plenty, I eat just enough, I could eat more, I don’t eat vegetables at all) |
| Double-barrelled questions (asking for more than one piece of information in a question) | Use separate questions for each piece of information |
| Do you think the community needs to improve the central and river public walkways? | Do you think the community needs to improve the river public walkways? |
| Ask leading questions | Make your questions unbiased |
| Which of the following do you believe is most responsible for the high cost of health care? (Physicians, Irresponsible health insurance companies, the federal government) | Which of the following do you believe is most responsible for the high cost of health care? (Physicians, health insurance companies, the federal government) |
| Double negatives | |
| “Do you not think that home care nurses have no time for questions? | Do you think home care nurses have enough time for questions? |
| Make assumptions | |
| Do you have extra money after paying bills that you invest? | This question would be better asked in two parts: do you have extra money after paying bills? (If yes: Do you invest the extra money you have after paying bills? |
Resources
- How to conduct a survey – Resource from Queensland Government, including information on survey types, sampling, question development and analysing responses
- Typeform – A webpage with tips for writing survey questions
- How to Create a Bad Survey Instrument – PMC (nih.gov) – An article about what not to do when writing surveys
Interviews
Pros
- Can be useful to explore specific issues in more depth than surveys
- Helpful for people that are not comfortable speaking in front a group
Cons
- Time consuming
- Interviewees may not be representative of larger community
Tips
- Tell the person you are interviewing how long it is going to take
- Offer to call back at another time
- Can invite either by directly calling people or sending an email/SMS/letter
- Once you have collected interview responses, sort the responses you get into categories or themes
- Get help or support from an experienced qualitative researcher
Writing interview questions
- Limit the number of questions
- Decide on how structured you want interviews to be
- Structured (you do not deviate from the script), semi-structured (there are scripted questions but some flexibility to explore topics that come up organically) or unstructured (completely open for the consumer to lead the discussion)
Resources
Some Strategies for Developing Interview Guides (harvard.edu)
- Guidelines for writing interview questions including a step by step guide
Focus groups and workshops
- Small group discussions around a specific topic.
- Hosted by a facilitator
- There are usually clear questions to answer and a clear scope of what the group needs to achieve within the session.
- Can have multiple sessions to focus on successive questions.
- Uses:
- Discover barriers, enablers and stakeholder needs in more depth to guide project planning
- Problem solving with the aim of developing recommendations or specific actions
- Educational sessions for building particular skills
- These are usually quick and fairly low cost, but do require a skilled facilitator.
Tips
- You can mix health professionals and consumers and each group will get good insight into the experiences of the other group. However, separating these groups may allow participants to feel more free to express negative experiences.
- Aim for 2 hours max. After that you will need to plan another session or factor in a break.
Example – Kidney Care Plan (submitted by Graeme Turner, Nurse Practitioner, Northern NSW Local Health District)
- Invites sent to Primary Care Nurses who were asked to invite a patient from their practice with Chronic Kidney Disease
- Workshop over dinner
- Sessions recorded on paper and on tape
- Follow up – drafts sent via email for feedback
Workshop
- Welcome, introductions, ice-breaker
- Explanation of how the workshop works
- Background information about problem/project (what is a care plan, why are they important, what do current plans involve?)
- Break for dinner and networking
- Session 1 – nurses and consumers separate (what are each group’s needs in regards to a care plan)
- Session 2 – participants mixed (deciding on the care plan format
Project steering/advisory groups
- Provide high level oversight including budgets and policy or process development
- Meets regularly to ensure consumer needs are considered at all stages of the projects (including advocating for other consumers’ needs)
Project working group
- Usually has more influence over the project.
- It may meet over a period of time, like a steering group, but with more influence over the day to day activities of the project
- E.g. new model of care or clinical guidelines, service redesign or evaluation, committees for awarding grants
Co-design
- Co-design is when all participants have equal decision making power as partners in whatever activity you are working on. It is a type of participatory design.
- Co-design is about seeking consumer and clinician leadership from the outset so that consumers and clinicians are involved in defining the problem and designing the solution.
- There will be times when co-design activities are not feasible. We can apply the principles and ideals of co-design to some parts of our projects and use other methods of engagement in other parts.
Is co-design appropriate for my work?
- Can all people involved be equally involved in decision making?
- Is the balance of power equal between staff and people with lived experience?
- Are all contributions genuinely valued?
- Which part of the project can you commit to consumers playing an equal role in – solution generation, design, delivery?
- Can you support people to take part in activities?
- Does your budget and timeline cover training and support?
- Have you allocated enough time (multiple sessions, research, development, feedback) for meaningful co-design?
Principles of co-design
- Shared decision making power
- Person-centred –understanding experiences and using this to design change
- Inclusive – draws on many sectors and perspectives and places equal value on all contributions
- Starts with the end/outcome that the group desires, not a list of what’s wrong
- Seeks to create practical, real world solutions
- Uses different methods and design-led processes to make ideas, experiences and possibilities visible and tangible to support active participation in the process
How to co-design
“Planning, designing and producing services with people that have experience of the problem or service means the final solution is more likely to meet their needs.”
“Co-design can be used to create, redevelop and evaluate a product, service or system. It can be applied to anything from an app to improve people’s accessibility, to major community service reform processes. It is not the answer for everything but can be effective when responding to complex issues.”
- It is not a one off event – occurs in stages or phases:
- Understanding people’s experiences of the issue and defining the issue
- Developing potential solutions
- Testing these ideas
- It is not linear. The process is cyclical and issues or ideas may have to be reassessed throughout.
- It cannot be rushed. It requires time and resources.
 May require multiple facilitators and orientation and training for consumers
May require multiple facilitators and orientation and training for consumers- Spend time making sure everyone involved has a clear understanding of the scope and intent of the process.
- Each method of engagement must have a way for capturing ideas and outcomes (e.g. dedicated note takers, writing ideas down and collecting, recording, photographs).
- Participants should be given the record of outcomes to review so they know their input has been captured correctly.
- Keep people in the loop about the outcomes of the co-design and the process.
- Evaluate the process as well as the outcomes (e.g. changes resulting from engagement, capacities being built, barriers encountered and solutions, learnings about the system, which methods of engagement work best, what risks needed to be managed).
- Celebrate the value of everyone’s contributions.
Co-design toolkit and information
- https://aci.health.nsw.gov.au/projects/co-design
- https://aci.health.nsw.gov.au/projects/co-design/working-together-with-aboriginal-communities
- https://metronorth.health.qld.gov.au/get-involved/co-design
- https://www.ncoss.org.au/wp-content/uploads/2017/06/Codesign-principles.pdf
- https://www.yacwa.org.au/wp-content/uploads/2016/09/An-Introduction-to-Co-Design-by-Ingrid-Burkett.pdf
- http://www.cocreate.training/wp-content/uploads/2019/03/co-design_handbook_FINAL.pdf
- https://www.orygen.org.au/Training/Resources/Service-knowledge-and-development/Guidelines/Co-designing-with-young-people-The-fundamentals/Orygen-Co-designing-with-YP-the-fundamentals?ext
- https://www.pwdwa.org/documents/connect_with_me/co-design-toolkit/index.htm
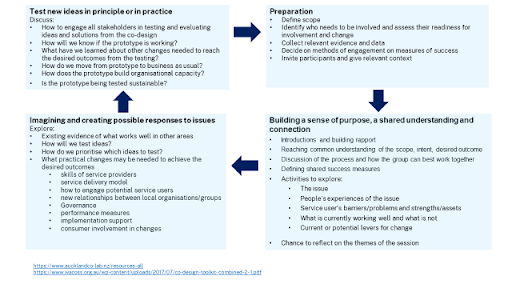
- https://www.aucklandco-lab.nz/resources-all
- https://www.mind.org.uk/workplace/influence-and-participation-toolkit/how/methods/co-design/
- https://www.wacoss.org.au/wp-content/uploads/2017/07/co-design-toolkit-combined-2-1.pdf



 Northern NSW Health Literacy Project acknowledges the traditional custodians of the lands across our region and pays respect to the Elders past, present and emerging. We recognise these lands were never ceded and acknowledge the continuation of culture and connection to land, sky and sea. We acknowledge Aboriginal and Torres Strait Islander peoples as Australia’s First Peoples and honour the rich diversity of the world’s oldest living cultures.
Northern NSW Health Literacy Project acknowledges the traditional custodians of the lands across our region and pays respect to the Elders past, present and emerging. We recognise these lands were never ceded and acknowledge the continuation of culture and connection to land, sky and sea. We acknowledge Aboriginal and Torres Strait Islander peoples as Australia’s First Peoples and honour the rich diversity of the world’s oldest living cultures.